COVID-19: So A lot Unhealthy Data
- Understand pandemics throughout history and what we have learned from them
- What the data really mean
- Let's talk about masks
- The important number that nobody talks about
- To go to school
- Using a natural anti-pathogen formula as prophylaxis to prevent the virus from ever occurring
- I'm looking forward to
If you come from a country where the coronavirus is somewhat under control, this newsletter is not for you. That said, don't hesitate to read it for entertainment value, but for the most part it doesn't apply to you.
Some stories
I had to rethink this newsletter a few times. There were coronavirus-related issues that needed to be investigated, but it has become apparent, especially since the last newsletter, that we have reached the limits of scientifically based arguments backed by studies. It turns out that bad information is even more contagious than the coronavirus, and there is no way to counter it. Science is no longer an effective antithesis when so many people believe that scientists are lying to them and instead believe in the most extreme theories spread on the internet. When it comes to COVID-19, people have staked out their territory and made camps based on their beliefs. There are people who automatically believe what scientists and medical experts say about the virus – even when they are repeatedly found to be wrong. On the flip side, there are those who choose not to believe the mainstream scientific community and follow the advice of more fringe experts, even if those experts also tell us that people get sick because they have sex with astral demons inside them Sleep and that vaccines are dangerous because they're made with foreign DNA (and no, I'm not talking about the aliens who migrate across the border to the US).
I planned to do my usual thing and write a newsletter with quotes and scientific references, but things have changed so much in the past three months. For a large part of the public, science is no longer an explanation of what is happening to the coronavirus. People are looking for a bigger, fuller, and fuller explanation for the chaos we are facing now – an explanation that is way beyond the reach of science.
Therefore a different approach is needed. Rather than discussing the science, I'd like to come up with a narrative that might shed light on how we view the facts on the ground. And the best place to start is with a little pandemic story. This is also a giveaway for me as I can cut and paste from the section on pandemics I just put together for rewriting the Miracle Doctors lessons. Incidentally, for those of you who are interested, I've now completed 28 of the 30 chapters in the book. With just two chapters left, the book now has more than 350,000 words and more than 1,700 clickable citations. I expect to be ready by the end of August. From this point on, I'll hand it over to editors for proofing and formatting for Kindle and Apple books, etc. This is expected to take 2-3 months. But enough about me.
Pandemics
Let's take a quick look at some of the major pandemics in human history to get a sense of how long they lasted, how many they killed, and how they ended.
Plague of Justinian (bubonic plague)
- Lasted 200 years (The majority of deaths occurred between 541 and 542, but this pandemic was persistent and only faded completely to 750.)
- Killed more than half of the world's population
- Ended when no one could be infected anymore. Half the world had died, the other half was infected, had survived, and was now immune.
Black Death
- The bubonic plague returned to Europe in 1347. It lasted about 300 years.
- In just four years, half of Europe's population was killed. The plague reappeared roughly every 20 years from 1348 to 1665–40 in 300 years. And with each new plague epidemic, 20 percent of the men, women and children living in London have been killed.
- It essentially ended with locking up the sick so they couldn't infect the healthy and burying the dead in mass graves.
Smallpox in the New World
- Smallpox has been endemic to Europe, Asia, and Arabia for centuries. It killed 30% of those infected and left survivors with pockmarked faces. It was brought to the New World with the first European explorers in the 15th century. The indigenous peoples faced no resistance. For them it was a "new" virus.
- Over the next hundred years, it wiped out 90-95% of the local population. In Mexico, the population decreased from 11 million before the conquest to just one million. Smallpox in the New World is by far the deadliest pandemic in human history.
- It ended when there were no more Native Americans to infect.
- The smallpox vaccine, introduced by Edward Jenner In 1796 the first successful vaccine was developed. It took 200 years of vaccinations to eradicate smallpox. In 1980 the World Health Assembly declared smallpox eradicated. Since then, no cases of naturally occurring smallpox have occurred. Other pathogens, such as bubonic plague, have seen ebb and flow throughout history, but smallpox is the only pathogen that has ever been cleared from the earth!
- We got very close to polio, but the fear of vaccinations in some countries in Africa and Asia is causing the number of cases to rise. One worrying thought is that if the disease breaks out from a handful of countries that contain it now, no one in the developed world will have more immunity to the disease. It would spread quickly.

cholera
- Cholera originated in the Ganges Delta in India.
- It spread around the world in the 19th century. Six subsequent cholera pandemics have killed millions of people on every continent. The current (seventh) pandemic began in South Asia in 1961 and reached Africa in 1971 and America in 1991. She is still active.
- In the mid-19th century, cholera killed tens of thousands in London. John Snow, a British doctor, found it was transmitted through contaminated water. In particular, people were infected with drinking water contaminated by sewage near the infected wells. The improvement of urban sanitation in the industrialized countries brought an end to the cholera pandemics in the industrialized countries. Unfortunately, it's still a persistent killer in third world countries due to a lack of adequate wastewater treatment and access to safe drinking water.
HIV / AIDS: Sub-Saharan Africa
- 1981 until today.
- Between 56 and 100 million people have become infected with HIV since the pandemic began. (Note: WHO actually defines HIV as a “global epidemic,” whatever that means. Between 25 and 42 million people have died of AIDS-related diseases since the epidemic began.
- It's far from over, but HIV can be treated well in developed countries so that it doesn't lead to AIDS. Even so, AIDS is still incredibly deadly in developing countries without access to adequate health care and preventive measures.
Spanish flu
- There have been a number of deadly flu outbreaks over the years, but the 1918 Spanish flu is the worst in history. Although the Spanish flu is mentioned, scientists are largely certain that it didn't start there. The best guess is that it came from the United States, with China making a strong runner-up.
- It is estimated that 500 million people, or a third of the world's population, were infected in just two years. It is also estimated that 40-50 million died.
- There were no vaccines and no therapeutics. In the end, it disappeared as a result of wearing masks and social distancing.
What did we learn about pandemics?
Yes, all pandemics eventually end, at least for a while. But not all pandemics end like the flu in a few months. Many can go on for hundreds of years before "magically disappearing" – just to win back each generation, while herd immunity disappears with the next generation to keep striking. While we cannot eliminate most pandemic pathogens, we have some great advantages over the ancients.
- We can understand much better how pathogens infect, spread, and kill.
- This enables us to implement guidelines that will inhibit their ability to spread and develop therapeutics that can significantly lower the death rate or even help patients live for decades during infection. People who are infected with HIV can now usually live indefinitely free of symptoms. And in the past six years, newly developed therapeutics have reduced the death rate for Ebola from 74% to just 6% if treated early enough.
- We also have options for testing and tracking contacts on a large scale that were not available to people in the past.
- And despite the resistance of many to their use, vaccines are sometimes available with varying degrees of effectiveness (20% to 90%, with benefits ranging from just a few months to several decades) and side effects (from mild to occasionally fatal).
With the flowering of human civilizations, infectious diseases also blossom. It is the inevitable result of large numbers of people living in close proximity to one another – and to animals – often with poor hygiene and nutrition. This provides fertile breeding grounds for disease. In ancient times, overseas and onshore trade routes slowly spread novel infections from country to country, causing the first global pandemics. Today it is international air traffic that can spread a pandemic to the other ends of the world within a few hours!
To conclude, here is a list of the tools we now have available to help fight pandemics.
1. Vaccines
A low-risk, effective vaccine is the most efficient way to stop the spread of a pandemic. Unfortunately, that's easier said than done. In all of human history, only one pandemic has been wiped off the ground by a vaccine. Every other vaccination program has lagged behind in terms of effectiveness and / or lack of harm. Some highly effective vaccines have done significant damage at different times in the course of their development. In particular, I am talking about the polio vaccine. Yes, it is highly effective now and is close to wiping polio off the floor, but along the way, versions of the vaccine caused both polio and brain cancer in patients until those problems were discovered and resolved. To be clear, none of these issues are present in current iterations of the vaccine – but they were at one time.
The other problem with vaccines, of course, is how to convince people to use them. According to a national survey designed and analyzed by the Tufts University Research Group on Equity For Health, Wealth, and Civic Engagement, only 57% of Americans say they would receive a COVID-19 vaccine when it became available would. This is not enough to develop herd immunity.
Of course, no vaccine for COVID-19 is currently available. We have no idea how effective any vaccine in the pipeline will be. And we have no idea what side effects this could have on the general population. Still, there is a political need to inject a vaccine into everyone's arm as soon as possible, reducing the evaluation time from 18 months to just six months. What could possibly go wrong when a vaccine is developed at warp speed?
2. Testing, quarantine and contact tracing

This can be very effective. Countries like South Korea and all of the Nordic countries took advantage of this to great effect during the coronavirus pandemic. If you can fast Test for possible infections, quarantine for anyone who tests positive, and then track and quarantine anyone who has been in direct contact with the infected personyou can control a pandemic with minimal discomfort to the general population. In fact, this method alone has kept the infection rate so low that only 5-10% of citizens in the Nordic countries struggle to wear a mask in public places, a number that has remained stable since the outbreak began.
In the US, this is no longer an option.
- We got into the test match late.
- We have been in the pandemic for five months and do not yet have adequate per capita tests.
- Test results for most people take far too long to be useful when it comes to quarantine or contact tracing.
- The accuracy of many tests has been dubious, at least so far.
- Too many citizens in the United States are considering tracking down a violation of their personal freedom and refusing to cooperate with the authorities. Using a mandatory phone app that makes contact tracking easy, automatic and requires minimal manpower is not a novice in the US for privacy reasons. And to tell the truth, given the government's track record in policing its citizens and invading their privacy, I can't say I disagree. However, for the countries that used them, these apps have been extremely effective in limiting the spread of the virus without the need for an army of trackers and general bans.
- Even if we wanted to now, we have allowed the pandemic to get so out of hand and infect so many people that it would be impossible at this stage of the game to have effective testing, selective quarantine and contact tracing programs.
- The president doesn't like any aspect of testing, quarantining, or contact tracing – so this is likely a non-starter at least at the national level right now.
3. Social distancing
The idea of the American State of Emergency is built into our culture. It has always been linked to the idea of freedom. The identification of the United States as the unique embodiment of freedom in a world flooded by oppression dates back to the American Revolution. It served us well when it comes to things that benefit from innovation, unconventional thinking and entrepreneurship. Think about business, science, entertainment, and technological innovation. If we had a political discussion I would start a discussion now about how it affects our view of the world and our relationships with other countries around the world, but that's for another day and another writer. The problem for us today is that the American state of emergency also has a disadvantage. It serves as a justification for people to take steps for the good of society as a whole in the name of their personal freedom. Here's a picture of Coney Island on July 4th – no social distancing and no face mask in sight. What else has to be said?

4. Masks and other PPE
If you've already eliminated vaccines, testing, quarantines, contract tracking, and social distancing as options, masks are the next line of defense. Unfortunately, 30% of Americans say they either sometimes, rarely, or never wear a mask when they leave the house. At this non-compliance rate, the virus spreads quickly. (We'll talk more about masks later.)
5. Lock
Lockdowns are the last line of defense. If people don't follow the guidelines mentioned earlier, you'll end up giving orders for entire churches to stay home and lock up indefinitely. Just a few days ago, the president said that "bans will not prevent future infection," and he is absolutely right. I said the same thing in early March. (You wonder if he's reading my newsletters now.) Since no one gains immunity in lockdown, this approach is just to buy you time. Time to prep hospitals and spread infections so your medical response isn't overwhelmed. But once you lift the lockdown, the pandemic is likely to build up as people break out of their homes and break all the rules in an orgy of "liberation". (See picture above.) Also, mass bans are incredibly disruptive to life, mental well-being, employment, and the economy. You are a well that can only be drawn so many times before people refuse to stick to it. We are probably already at this point.
6. Natural herd immunity
This is what happens when everything else you've tried has failed. There are three problems with this:
- It can take a long time. It took 200 years for natural immunity to take hold during Justinian's Plague.
- It can be costly in terms of human life. When smallpox pierced the indigenous peoples of North and South America, over 90% of the population died before the 10% who survived the disease gained herd immunity and horrific disfigurement.
- It doesn't last. People have this nasty habit of making copies of themselves. The problem is that the copies (often referred to as children) don't share their parents' immunity and thus the pandemic can keep recurring. As we saw with the Black Death, in 300 years the plague reappeared roughly every 20 years from 1348 to 1665/40. And with each new plague epidemic, 20 percent of the men, women and children living in London have been killed.
7. Wait for the pandemic to magically disappear

The belief that pandemics magically disappear as part of their natural cycles is mostly incorrect for two reasons.
- So far, no pandemic has permanently disappeared on its own without human intervention. Many have walked for hundreds of years and then disappeared, only to reappear years later. This is mainly the result of dwindling herd immunity.
- Some, like the flu, seem to magically go away every summer and come back every fall. This is the result of a virus mutation that makes existing herd immunity superfluous.
The only pandemic that has completely disappeared is smallpox, and that was not the result of a magical disappearance, but the result of developing a vaccine.
8. Therapeutics
Therapeutics are essentially what we do when we can't get rid of the pandemic. HIV is a good example. We cannot stop the virus from spreading just yet, but through the use of therapeutics we have succeeded in converting a particular death sentence into decades of relatively normal life. We have learned to coexist with the pandemic.
The data
A big problem we are facing now is that many people are questioning the numbers they see on the news. They believe that the death toll is well below the numbers shown on television. Almost one in three Americans is skeptical of the official death toll, according to a July 21 poll. They consider the coronavirus pandemic a joke. The main claim is that hospitals are adding to the numbers by claiming that if someone dies of a heart attack but is only in contact with someone who has had COVID-19, the hospital will list this as death from COVID-19, not a heart attack because they get more reimbursements for coronavirus deaths. Nor does it help that the president keeps saying that if fewer tests were done, the numbers would be lower.
Surprisingly, both of these claims are partially correct. Although they contain an element of truth, the parts that are not true make them highly misleading and completely irrelevant.
How to determine the cause of death
Let's start with how hospitals determine the cause of death. Big surprise everyone, nothing new here. Hospitals have been doing this all the time and for years – and no, so as not to ask for a higher reimbursement. It's very easy; In most of the cases when someone dies there are comorbidities. Let me give you a very common example. Someone's got the flu. It causes inflammation of the lung tissue and weakens the immune system. This opens the door for them to catch pneumonia. Pneumonia inflames your arteries and destabilizes plaque on the artery wall, which then loosens and creates a blockage that leads to heart attacks and death.
So what does the doctor list on the death certificate: flu, pneumonia, arterial inflammation, plaque, arterial blockage, or heart attack. Guess what: there is a protocol for that. It is called the "underlying cause of death" which is defined as illness or injury that initiated the train of events that lead directly to death. In this case, influenza is listed as the underlying cause of death on the death certificate.
And so, regardless of pre-existing comorbidities, COVID-19 is listed as the underlying cause of death – because it set off the "train of events" that led directly to death. Make sense? There's no bloating of numbers here. This is how the cause of death has been determined for years.
Well, to be clear, there are examples of states and / or hospitals:
- Marking some deaths as COVID-related, even when an alternative cause is clearly the more likely underlying cause.
- Marking any death in which someone tested positive for the virus as a COVID death, even if the actual cause of death was completely unrelated, e.g. B. a car accident or suicide.
- And sometimes labeling deaths as COVID-related even when post-mortem tests later showed the deceased never actually had the coronavirus.
However, this seems to be the exception rather than the rule. However, these "misjudgments" do not result in as many deaths. It should also be remembered that we now know that the coronavirus made its way through the United States for at least two months before we knew it was here. That means several thousand people likely died from COVID-19 before we even knew we should look for it, which means all of those deaths were attributed to a different underlying cause – most likely the flu – when in fact it was Case was the coronavirus that killed them. In other words, before you say the number of deaths from coronavirus in the US is overstated, you need to put those uncounted deaths back on your list as the official count may actually be undervalued.
The bottom line is that regardless of the exact number, we can generally clearly say that too many people have died from COVID-19.
The more you test, the more cases you will find
The president is absolutely right. It is 100% true that the more people you test, the more cases you will find. However, if you close your eyes and don't see cases of coronavirus, it doesn't mean they aren't there. More importantly, withholding testing not only makes the virus spread much faster and reach far more people because you're flying blind, it also makes another, even more important number look much worse: the incidence of mortality .
Let's just do it. If you test 1,000 people and 100 test positive for COVID-19 and 10 people die, you will see a death rate of 10% (10 out of 100 people who test positive). Conversely, if you had tested 10,000, you would have found ten times as many, or 1,000, that tested positive for the virus. (This is the number the President doesn't like.) Deaths have nothing to do with testing, however. In other words, you'd still have the same 10 deaths, which means your death rate would drop to just 1%. In other words, as more tests get more positive results (a bad one from the president), your death rate goes down (a good community good).
To put it simply, withholding tests is a bad idea. Flying blind through a major pandemic is a bad idea.
Although cases are increasing, deaths are not
With the incidence of COVID-19 rising sharply in recent weeks, the number of deaths per day has not kept pace. There can be several reasons for this.
- Increasing testing results in more cases, which, as we just discussed, ipso facto lowers the death rate.
- Reinforced tests lead to milder cases.
- Younger people now make up a larger proportion of the cases. And although they die, they die less often than seniors.
- Doctors now have therapeutics like Remdesivir the are proven to lower death rates and speed recovery.
- And the president may be half right again. He said warmer temperatures would magically make the virus go away. In warmer temperatures, the virus certainly hasn't gone away, but the virus may be less virulent. If so, unfortunately we can see to it that this benefit disappears in the fall, which means that the death rate rises again, if only slightly, as the temperature drops. Even so, COVID-19 doesn't appear to be a seasonal virus like the flu. Instead, it seems much more oceanic – just a continuous series of wave after wave after wave – that never really go away.
When we talk about deaths, we now get a partial answer to a question I asked in my last newsletter: How many deaths a day are we ready to tolerate before everyone in the country says, "Enough is enough?" Well, we have now hit 1,000 a day and this response has not yet been triggered. We now know that whatever it is, that level is going to be way higher than 1,000 a day.
When it comes to COVID-19 in the US we are terrifyingly seeing a frog in the water scenario. I'm talking about how a frog leaps out of boiling water but can be boiled alive if the temperature is slowly increased one degree at a time. If the deaths had risen from one to a thousand a day in March that month, there would have been panic and a national outcry. But by adding a few deaths every day over five months, we now seem to accept a thousand a day as just another fact of life that you live with. And when things keep picking up a little, there's no telling how high that number could be without causing national outrage.
Masks
Now let's talk about masks. Dr. Fauci now says that you should wear a mask every time you leave your house, and he also recommends adding safety glasses, face shield, and gloves to the mix. I understand the intent of the new guidelines: keep things as simple as possible (wear a mask when away) and maximize protection (use anything). And yes, more is better, but not necessarily that much better. We are talking about the law of falling returns here. And given how resilient so many people are to wearing a mask in any situation – let alone adding face shield and goggles – these new guidelines are likely to be followed even less religiously than previous guidelines.
Look, something is going on here and it is crossing political boundaries. It's visceral and anger-fueled.
In the 1918 flu pandemic, there were no vaccines and no effective therapeutics. Lockdowns, social distancing, and masks were the main defenses against the spread of the pandemic. Sound familiar? And of the three – hold on to your hats – masks were the most hated and the most resisted by the public. In places where mask commands were successfully implemented, non-compliance and outright defiance quickly became a problem. It's really true, isn't it: the more things change, the more they stay the same?
What has changed, however, are the arguments against the use of masks. In 1918 things were simple. People didn't like how they felt. The workers felt too uncomfortable to be carried all day. They "let their noses go to sleep". The arguments against them are much bigger today.
Let's deal with them quickly.
- Sie zwingen dich, deine eigene Luft zu atmen, dir Sauerstoff zu entziehen und deinen Körper mit Kohlendioxid zu vergiften. Dies ist nur geringfügig wahr. Luft nimmt Platz ein. Wenn Sie einen Ballon sprengen, während Luft den Raum füllt, wird der Ballon größer. Wenn der Ballon nicht größer wird, strömt keine Luft in den Ballon. Das heißt, wenn Ihre Maske nicht größer wird, kann nur „verbrauchte“ Luft aus Ihrer Lunge an den Stellen zwischen Maske und Gesicht gespeichert werden. Für weiche Masken, die nahe am Gesicht sitzen, gibt es einfach nicht viel Platz zum Halten der gebrauchten Luft, um wieder eingeatmet zu werden. Harte Masken wie N95, die aus dem Gesicht herausragen, halten definitiv etwas verbrauchte Luft in dem Raum, in dem die Maske aus Nase und Mund herausragt. Aber schau dir nur den Raum an; es ist nicht viel, aber es ist definitiv etwas.
![]()
- Masken „aktivieren“ das Virus und machen es ansteckender. Ja, ich weiß nicht wirklich, was ich dazu sagen soll. Es ist keine Sache. Es ist nicht real. So funktionieren Viren nicht.
- Masken enthalten Viren, wenn Sie sie berühren, damit Sie sie später einatmen können. Nicht wirklich. Viren wandern auf Wassertropfen. Wenn ein infiziertes Tröpfchen auf Ihrer Maske landet, wird das Wasser von der Maske absorbiert. Dies bedeutet, dass das Virus jetzt auf der Maske sitzt und nur durch direkten Kontakt und nicht mehr durch Atmen bewegt werden kann.
- Masken schützen dich nicht. Absolut wahr. Wie ich bereits im Februar sagte, bieten Masken dem Träger wenig Schutz. Sie behindern die Ausbreitung von Wassertröpfchen, die aus Ihren Lungen ausgestoßen werden, wenn Sie atmen, sprechen, schreien, husten oder niesen – und damit verhindern, wie weit sich die auf diesen Tröpfchen wandernden Viren bewegen können. Ungehindert können diese Tröpfchen in wenigen Sekunden Feuchtigkeitströpfchen aus Ihrer Lunge einen halben Meter weit reiten. Von einer Maske behindert, bewegen sie sich nur etwa 18 Zoll. Das ist der Grund, warum ein Abstand von zwei Metern und das Tragen einer Maske die Ausbreitung von Infektionen verhindern.
- Sie sind eine Verletzung der persönlichen Freiheit. Sie sind gut für diejenigen, die sie tragen möchten, aber es sollte eine persönliche Wahl sein. Das wäre wahr, wenn wir über den Schutz des Trägers sprechen würden. Aber wir sind nicht. Wir sprechen über den Schutz anderer vor einer Infektion durch Sie. Zu sagen, dass das Tragen einer Maske eine persönliche Entscheidung sein sollte, ist wie zu sagen.
- Trinken und Fahren sollte eine persönliche Entscheidung sein.
- Feuer in einem Theater zu schreien sollte eine persönliche Entscheidung sein.
- Es sollte eine persönliche Entscheidung sein, in eine überfüllte Nachbarschaftsbar zu gehen, während man mit Ebola infiziert ist.

Auf der anderen Seite ist das Tragen einer Maske, wenn sie nichts bewirkt – und tatsächlich Aktivitäten erschwert – fraglich und führt zur Nichteinhaltung.
- Orte, an denen man eine Maske tragen kann:
- So ziemlich überall drinnen außerhalb Ihres eigenen Hauses, wo andere Leute anwesend sind.
- Überall im Freien, wo Sie sich nicht sozial fernhalten können.
- Orte, an denen das Tragen einer Maske nur einen geringen Nutzen bringt:
- Im Allgemeinen im Freien – solange Sie sich sozial fernhalten können.
- Während Sie alleine im Freien trainieren, Rad fahren oder laufen. (Hinweis: Wenn Sie mit dem Fahrrad laufen oder laufen, können Sie einen Windschatten von Tröpfchen hinterlassen, der bis zu 30 m hinter Ihnen herläuft. Sie neigen jedoch dazu, sich in der Luft so zu zerstreuen, dass sie nur minimal ansteckend sind.)
- Jede Arbeitssituation in Innenräumen, die Ihre Atemfrequenz erheblich erhöht (in diesem Fall muss Ihr Arbeitgeber 12 Fuß soziale Distanz zwischen den Arbeitnehmern berücksichtigen).
Letzter Gedanke. Wie wir bereits besprochen haben, sind wahrscheinlich nur sehr wenige Personen in der Öffentlichkeit infiziert und infizieren möglicherweise andere, und es besteht die Notwendigkeit, überhaupt Masken zu tragen, wenn Sie das Virus mit ausreichenden Tests, Kontaktverfolgung und sozialer Distanzierung unter Kontrolle haben minimal. Und wie wir in den nordischen Ländern sehen, tragen nur sehr wenige Menschen Masken, und sie haben kein Problem. Leider sind die USA nicht in dieser Position. In den USA bieten Masken die letzte Verteidigungslinie. Wenn sich genug Menschen in den USA dafür entscheiden, keine Masken zu tragen, stehen wir vor einer erweiterten Welt voller Verletzungen.
PS: Since masks tend to reduce droplet travel to about 18 inches, they will not be effective if you can’t also keep socially distant.
William Henry Gates III
Poor Bill Gates. Back in 2011, he was accused by conspiracy theorists within the alternative health community of claiming to want to use vaccines to kill off 1 billion children, which, of course, is not what he said at all…or did.

Now, he is being accused of trying to use COVID-19 medical and dental injections to implant tracking chips. I mentioned this “theory” in my last newsletter and received several strongly worded emails accusing me of being naïve and not understanding the truth behind the accusation. In fact, according to a poll, fully half of all Americans who name Fox News as their primary news source believe the story that Bill Gates is looking to use a coronavirus vaccine to inject a microchip into people and track the world’s population.
But here is a surprise, the poll found that 15 percent of MSNBC viewers also believe this conspiracy theory. They chose to target Gates specifically because of his decade-long advocacy for vaccines.
So, just for fun, I decided to trace this narrative back to its source. And guess what: I found it. As Reuters Fact Check reported:
“This claim was originally posted as satire on May 13, 2020. Its author, Sam Powell ( here ) later described the post on his Facebook profile as “a wild exaggeration of false rumors already circulating” about Bill Gates and microchips.
“I stretched it to a ridiculous extreme to demonstrate just how willing the right wing extremists are to believe slanderous manipulations of the irrational fears of the anti-vaxxer community to demonize the allegedly liberal Gates and support their false tin idol Trump”, Powell wrote on Facebook, describing the post as a “subtle parody” ( here ).
He is a tad more demonizing of the right than I would like, but it doesn’t change the facts behind what happened next. The parody gained legitimacy and exploded when Fox primetime host Laura Ingraham shared a tweet where she expressed agreement with a user who wrote about the debunked conspiracy theory. She wrote, “Digitally tracking Americans’ every move has been a dream of the globalists for years. This health crisis is the perfect vehicle for them to push this.”
Thanks to Ingraham’s endorsement, different iterations of the claim have now been shared thousands and thousands and thousands of times. Examples of the post are visible here and here.
So, there ya go! I realize the information will not change any of the minds of those who are now emotionally invested in the theory. But at least you now know that it started as parody and how it gained legitimacy. So, there is that.
There Is an Important Number that No One Is Talking About

All the talking heads and politicians talk about testing, the number of people who get COVID-19, and the number who die. Or as the President likes to say, “99 percent of virus cases are harmless.”
But that’s not true. There’s an extremely important missing number here.
First of all, to be precise, the official mortality rate in the U.S. is not 1% as the President claims. It is 3.4%. But that’s because we don’t test enough. As I mentioned earlier, the mortality rate would go down with adequate testing. In fact, when all is said and done, the real mortality rate for COVID-19 is probably as low as 0.6%–especially now as more therapeutics like remdesivir come into play. But that does not mean the President is correct.
When it comes to COVID-19, we cannot limit our discussion to living and dying. This virus has significant morbidity even for those who do not die. About 40 percent of adults in the U.S. have at least one underlying health condition that would put them at risk for severe complications of COVID-19, according to a report published by the Centers for Disease Control and Prevention. The bottom line is that some 20% of those who come down with COVID, although they survive, find that the virus is anything but harmless. Many people, even young people, get extremely ill, and their road back to health includes weakness, shortness of breath, loss of muscle mass, and sometimes strokes. As we have discussed previously, COVID-19 can cause brain inflammation, hallucinations, psychosis, delirium, and nightmares. It can scar the lungs horribly, lead to weight loss and loss of lean muscle mass and has even been responsible for strokes in those age 40 and younger and loss of legs due to blood clotting issues. This virus not only affects the lungs and blood, but also the kidneys, liver, and brain–the last potentially resulting in chronic fatigue and major long-term depression, among other symptoms. It may not kill a high percentage, but it does still ravage a significant percentage of people.
A Dutch report published in early July (an excerpt is translated here) surveyed 1,622 Covid-19 patients with an average age of 53 who reported a number of enduring symptoms, including intense fatigue (88%), persistent shortness of breath (75%), and chest pressure (45%). Ninety-one percent of the patients were not hospitalized, suggesting they suffered these side-effects despite their cases of COVID-19 qualifying as “mild”. While 85% of the surveyed patients considered themselves generally healthy before having COVID-19, only 6% thought so one month or more after getting the virus.
Conservatively, you are looking at 10 times the number of people who die from COVID-19 having long-term health issues. When you add in those who suffer long-term harm from the virus, we’re not talking 160,000. We’re talking several million people. So no, it is not “harmless” for 99%.
Children and Schools

There is a passionate, raging debate right now when it comes to opening schools. There are parents and teachers on both sides of the question. Some of it is political, but I’m not going to go into that side of it. I just want to talk about the safety aspect.
On the open now side, there are two main points.
- There is some evidence that children are less likely to catch the virus versus adults, and when they do, they are less likely to get as sick. Although the evidence leans in that direction, it is ambiguous at best, and even if true, it only applies to children under 10. At 10 and up, their susceptibility is the same as any adult’s. But even for younger children, “less likely” does not mean “not at all.”
- There is also evidence to suggest that children are also less likely to transmit the virus VS adults. Again, the evidence is highly ambiguous–and again, if true, only for children under 10. At 10 and up, their communicability is the same as any adult’s. And again, even for younger children “less likely” does not mean “not at all.”
On the stay closed side, there are the facts on the ground.
- Two weeks after Israel fully reopened schools, a COVID-19 outbreak swept through classrooms — including at least 130 cases at a single school.,
- A summer camp in suburban Dallas was forced to close less than two weeks after opening when both children and counselors showed symptoms and tested positive for COVID-19. The camp had put numerous safety precautions in place, including mask wearing, daily temperature checks, social distancing of age groups, no food or material sharing, and much more. Similar outcomes were seen in Oklahoma and Missouri where dozens caught the virus.
- Several weeks ago, 260 of the 597 children attending a summer camp in Georgia contracted the coronavirus, adding to a growing body of evidence that minors are both susceptible to infection and serve as vectors of transmission. According to the CDC, the true number of infected campers was probably significantly higher since test results were only available for 58 percent of the group.
- As of June 30th, there were 950 reported positive cases of COVID-19 in Texas at 668 childcare locations–307 children and 643 staff members. Statewide, 12,207 licensed childcare operations were open at the time, and total reported coronavirus cases had risen from 59 cases in mid-May and 576 on June 23.
- One of the first school districts in the country to reopen its doors during the coronavirus pandemic did not even make it a day before a call from the county health department notified Greenfield Central Junior High School in Indiana that a student who had walked the halls and sat in various classrooms had tested positive for the coronavirus. “We knew it was a when, not if,” said Harold E. Olin, superintendent of the Greenfield-Central Community School Corp., but were “very shocked it was on Day 1.”
- And finally, a study published online in JAMA Network found that infected children have at least as much of the coronavirus in their noses and throats as infected adults, according to the research. Indeed, children younger than age 5 may host up to 100 times as much of the virus in the upper respiratory tract as adults.
And then there are the teachers.
- Thirty percent of elementary school teachers are age 50 or older, which puts them in a high-risk group.
- In mid-July, a longtime Arizona elementary school teacher died of coronavirus after sharing a summer classroom with two other teachers who also fell ill with the disease. They were teaching virtual summer school lessons, and the educators “took extra precautions” and “followed the CDC guidelines and more,” but still got sick. They kept their distance, wore masks, and constantly used hand sanitizer.
- At least 600 Florida teachers have requested living wills as they prepare for schools in the state to reopen even as coronavirus numbers swell.
So, let’s cut to the chase. The primary argument I hear in favor of opening schools is that other countries all over the world are safely opening schools (not counting Israel and France, of course), so why shouldn’t the United States?
And the simple answer is lava!
When lava is hot and fresh and flowing, it’s not a good idea to walk on it. Once it has cooled, though, there is no problem walking on it. In fact, if you wait long enough, after the lava breaks down into volcanic soil, the lava field is not just safe to walk on, it is absolutely verdant.


So, the simple answer as to why other countries can safely open schools and we cannot in the many, many areas of the country that currently have high infection rates is that they are opening their schools on a cooled lava field, whereas we are trying to open them (at least those in the “hot” districts) on flowing lava fields–metaphorically speaking. (See table below.)
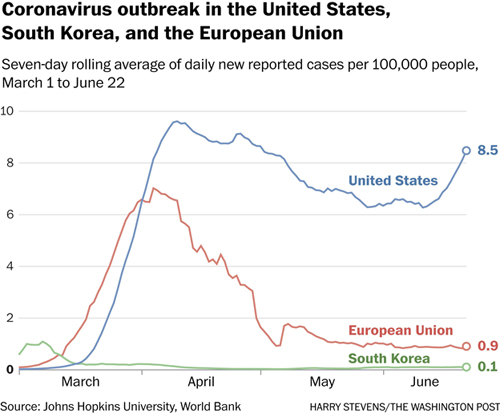
Note: in the above chart, the numbers are not affected by the number of tests. The numbers reflect an average per hundred thousand people. If you test 100,000, 200,000, 1 million people, it doesn’t matter. While the total number of people with the virus would indeed go up, that number never appears in the chart–only the average per 100,000, which would remain unchanged.

Natural Antipathogen Formula as a Prophylactic
One of the things I was challenged on in my last newsletter was that several months earlier I had said there was no need to panic, and now I was preaching doom and gloom and large amounts of dead people. In fact, nothing has changed. I have said from the very beginning that I expected a large number of deaths–and those predictions are proceeding apace. Specifically, what I said is that the coronavirus had a low mortality rate, but that a low rate applied to a large susceptible population (essentially every person living in the United States) would mean a large number of deaths. But what I also said was that there was no need to panic since there are steps you can take that will likely put you on the good side of those numbers. And one of the more essential pieces of that program is an effective natural antipathogen formula.
Since I first mentioned that formula, many people have written in to ask if the natural antipathogen formula could be taken on a daily basis in smaller amounts to prevent ever getting the virus in the first place. The idea would be to use it prophylactically versus waiting until you experience the first symptoms and taking it in larger amounts to throttle back its progression from that point?
That’s an interesting question.
Before we go any further, we need to keep in mind that there is no actual proof that the formula works to kill the virus if you have been infected. Yes, there are thousands of anecdotal testimonials over the years as to how well it works in controlling the flu, but none of this constitutes proof. Without the rigors of a large cohort study, there is no proof that people who didn’t use the formula wouldn’t have had exactly the same experience in terms of either preventing the flu from hitting full on or patients getting well in what appeared to be half the time. And when it comes to the coronavirus, we have far fewer anecdotal reports. There is me, Kristen, and maybe a half dozen others who have written in to say that the formula prevented the virus from progressing. But with the coronavirus, the same might have been claimed by 80% of people who came down with the virus, took nothing to mitigate it, and had no or very mild symptoms.
And if we ever did run a huge cohort study and proved the formula stopped COVID-19 in its tracks, I couldn’t talk about those results. If I did, the formula would be classified as a drug and could only be sold by prescription. And Baseline Nutritionals has no network of pharmaceutical reps to convince doctors to do so. In other words, Baseline would no longer be able to sell the formula.
So, where does that leave us?
For the thousands of people who have used the antipathogen formula over the last two decades, they do not need any studies. Based on their personal experience on multiple occasions, they are convinced the formula works. And their experiences are the reason that months of inventory for that formula was cleaned off the warehouse shelves in a matter of days back in March when people suddenly realized the coronavirus was for real. Which brings us to the question at hand: instead of just using it after you notice symptoms, can you use the antipathogen formula prophylactically to prevent ever getting the virus in the first place?
And the answer is: possibly, yes, theoretically?
Again, although there are many reasons to suspect it might work well for this purpose, there are no studies that prove it does so. In fact, such studies would be almost impossible to conduct. When it comes to assessing protection potential, you are talking about a large cohort study in which you analyze the data from a large cohort of people who were exposed to the virus during the course of the study.
Then you compare the infection and mortality results of those who regularly used the formula with those who did not. Unfortunately, no such cohort exists, nor is there ever likely to be one. So, when it comes to the efficacy of using an antipathogen formula to prevent the virus, you are flying blind. Nevertheless, the formula contains several powerful antivirals, and we do have several decades of testimonials vis-à-vis the flu–so again, it’s theoretically likely. Which brings up the question: if so, how much do you need to take?
We already know that when you are dealing with an all-out infection, you need to take a bottle a day for three to four days until the infection is somewhat under control. After that, 10 droppers a day is sufficient. So, 10 droppers a day is a reasonable starting point. The problem with 10 droppers a day for prophylactic purposes, though, is that you are talking about 5 bottles a month, which would get expensive over several months. My guess, and this is just a guess, is that 5 droppers a day, two days on and one day off should do the trick, or at the very least make it likely that any infection is minimal. At that rate, each bottle would last about 18 days, so you are talking just under two bottles a month–which is a whole lot more economically feasible than five bottles a month.
Also, keep in mind that if you are using the formula that regularly, you will want to be sure to supplement with a good probiotic. Yes, the ingredients in the formula, although antibiotic, are gentle when it comes to your intestinal bacteria. But if you are taking it that regularly for weeks on end, it will begin to negatively impact your intestinal flora. So yes, you will want to supplement with a good probiotic to balance out that effect.
Looking Forward

Unfortunately, thanks to an incoherent response from the highest levels of government, inconsistent messaging from public health officials, the media giving diametrically opposed opinions (depending on what station you listen to), not to mention public antipathy for many of the mitigating recommendations, the fight against COVID-19 in the United States has begun to feel hopeless. As a result, conspiracy theories have replaced science for many, whereas others have simply thrown caution to the wind. Now, instead of working as one country to suppress the virus and emerge slowly and carefully into public life again, people are making up their own rules as they go. And the result is chaos, many more deaths than we should ever have seen, and savage disruption to our economy–not to mention an astonishing number of people who claim the entire thing is a hoax. Without leadership from the top, the national response is fragmenting.
- And if you are waiting for a vaccine, don’t count on it helping very much. If the new vaccines are 50% effective, like the flu vaccine in a good year, and only 50% of the population is willing to take it, we are going to be living with the coronavirus for a number of years to come.
- Some people will be immune because they have already had the virus.
- Some will be immune because they got vaccinated and it worked for them.
- Some will do nothing, take no precautions, refuse to wear masks and social distance, come down with the virus, and count on their doctors to use therapeutics to get them through.
- New therapeutics will help here
- And retail businesses and restaurants will find ways to reopen in the new environment by taking steps to kill the virus in the air and prevent its spread from person to person. For example, there are studies to show that air ionizers can kill airborne viruses. The problem is producing enough negative ions economically to sanitize an entire restaurant or store. And other studies have shown that far-UVC light can kill airborne coronavirus. Bottom line: there are ways to make the air and surfaces in indoor environments anathema to coronavirus transmission–without the need for masks.
- Some will have long-term side effects or die.
- And some will proactively build their immune systems and keep a supply of a good natural antipathogen formula on hand to handle any eventuality.
By default, and without consciously choosing it, the United States appears to be heading for a chaotic, slightly modulated, free fall descent into natural herd immunity. If you think I’m exaggerating, then consider that even as I write this, a quarter of a million bikers from every corner of the country are gathering in South Dakota for nine days for the 80th annual Sturgis Motorcycle Rally. And for those nine days, there will be no social distancing and no wearing of masks. As one of the bikers, Rod Woodruff told the Daily Beast on Wednesday, “We’re just celebrating good old American freedom.”
And they will be bringing whatever they catch in those nine days back to every corner of the country. We are so screwed!
Ultimately, it looks like we’re going to have to live with the virus for a long time. The only question is whether you choose to be proactive, reactive, or hope to hide from it. Some day, it would be nice to return to business as normal.

By the way, it’s probably worth mentioning that the long-term herd immunity thing (options 1-3) may not work out so well in the near-term as the virus is showing a propensity for mutation. At least one mutation made the virus 10 times more infectious. And a new strain that has just appeared in Vietnam appears to be both more infectious and more severe.
Note: There is one small positive here. With people working from home and a large number wearing masks and socially distancing (even if not enough to stop COVID-19), it should be enough to drastically reduce the spread of flu this year–ultimately dropping the influenza death toll by more than half.
Comments are closed.